It’s time to hang up the past.

It’s time to stop rewinding the past.

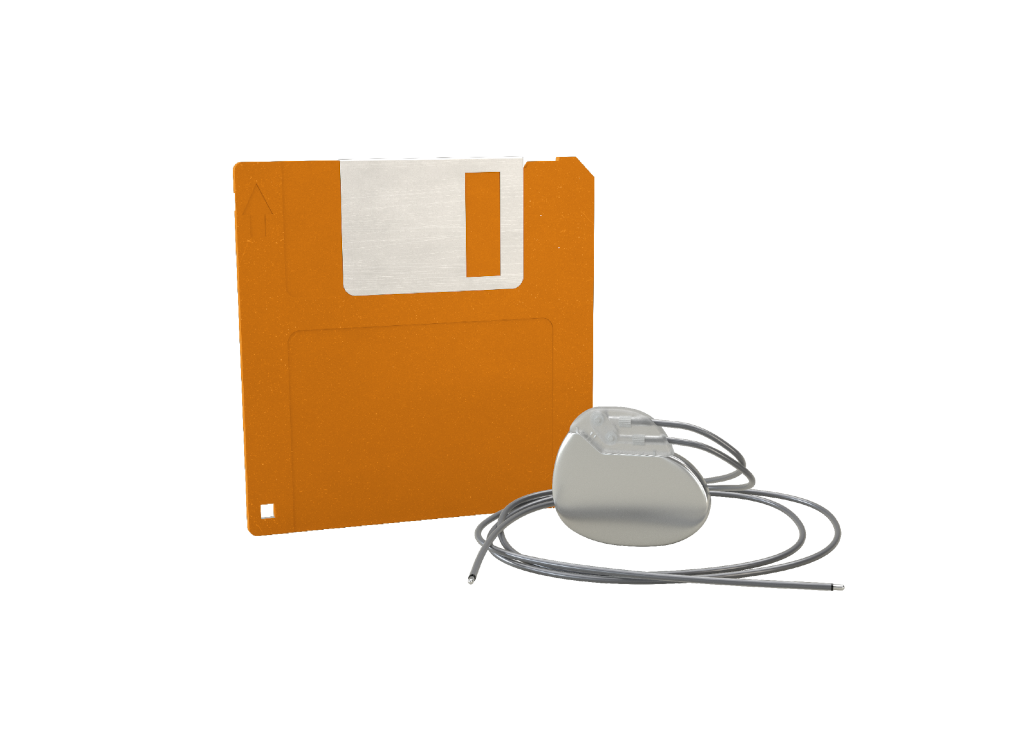
It’s time to eject the past.
It’s time to stop rewinding the past.

Leadless pacing isn’t a trend—it’s the next era of cardiac care. By establishing AVEIR™ Leadless Pacemakers as the standard in your practice, you offer patients a therapy associated with significantly fewer complications and reinterventions compared to traditional transvenous pacing. Lead with what’s next in cardiac care, starting now.

AVEIR™ Leadless Pacemakers result in fewer complications than transvenous pacemakers (TVP)
From implant to retrieval to repositioning, here are real-life cases presented by renowned experts in cardiac rhythm management and electrophysiology sharing insights and techniques on procedures for the entire portfolio, including AVEIR™ VR Ventricular LP, AVEIR™ AR Atrial LP and AVEIR™ DR Dual Chamber LP System.

“The adoption of a leadless-first pacing strategy has represented a paradigm shift in my practice.... Leadless pacing, particularly atrial leadless therapy, is now routinely offered as a first-line option for patients with pacing indications.”
From Leadless-First Pacing Strategy in Symptomatic Sinus Node Dysfunction: A Physician's Perspective

“You owe it to yourself and to your patients to master leadless pacemakers early in your career. As with any new procedure, there is a learning curve, and you must respect the differences.... The first thing to challenge and overcome is your own paradigm. Think about leadless pacemakers first!”
From Mastering AVEIR Leadless Pacemakers: A Physician’s Perspective on the Learning Curve

“AVEIR DR leadless pacing system is especially suitable for younger patients requiring a high percentage of AV Synchrony.”
From Dual-chamber leadless pacemaker outcomes in patients < 65 years of age

“The most physiologic form of pacing is no pacing.”
Deliver the most physiologic pacing strategy for your patient with a modular leadless system designed to treat a range of bradyarrhythmias. AVEIR AR2 Atrial LP, VR Ventricular LP and DR LP System offer chamber specific therapies, upgradeable pathways, and long-term retrievability.4


AVEIR™ DR DUAL CHAMBER LP SYSTEM
Our innovative leadless technology allows both atrial and ventricular devices to be implanted in the heart through a minimally invasive catheter-based procedure. A protective sleeve fully covers the leadless pacemaker during catheter navigation to reduce the risk of device damage and injury to cardiovascular structures.
References
MAT-2642377 v3.0 | Item approved for U.S. use.